The inclusion of Hyperbaric Oxygen Therapy (HBOT) in the treatment of Chronic Long-Term Lyme Disease (CLD), or the preferred term of the Infectious Diseases Society of America (IDSA) as “Post-Lyme Syndrome” (PLS) – Lyme Disease is controversial, even amongst physicians that have their own HBOT centers. Changes are being made constantly in treatment (Tx) protocols. Reasons for part-answers to the bullet point questions are given after scrolling to the base of this page …
Click on the questions below to see the answers
Should co-infections such as erlichia, barbesia, mycaplasma and bartonella be killed with pharmaceuticals before HBOT Tx. commence?
Some physicians say “yes”, others say “no”.
Read about the pathophysiology (the study of biological manifestations of disease and disturbance of health) of tick-bite co-infections to Borrelia bugdorferi (referred to as Bb), in the article Lyme Coinfections Hate Oxygen.
All of these “bugs” (bacteria and parasites) can be transmitted by ticks and other vectors. There is much debate and some confusion because of the incorrect assumption that HBOT will actually enhance some of these Bb coinfections. For example, because babesia canis (Bc) chooses red blood cells as a primary transport vehicle to infect the entire body, it is assumed that it does so because “it just loves oxygen.” This is not so as the Bc trophozoite cannot tolerate high oxygen tensions and HBOT will cause it to perish and will repair the microcirculation that Bc infections destroy. So too with the other coinfections.
HBOT, when administered at the appropriate treatment pressure, exerts a potent bactericidal and fungicidal effect and continues on to repair damaged cells, restoring normal organ function including neuronal circuitry. There is no doubt that HBOT act synergistically with many of the antibiotics (ABX) used to combat these co-infections and reduce the time these ABX needed for them to do their job.
Our observations are as follows:
• Some CLD/PLS patients are treated with HBOT along with oral or peripherally inserted central catheters (PICC lines) of antibiotics.
• Other CLD/PLS patients had previously been treated with various antibiotics, antifungal and quinine Rx … with poor results. They then had HBOT sessions with positive results.
• Yet other CLD/PLS patients had steadfastly refused to take antibiotics before HBOT, and had positive results.
• All of the CLD/LS patients underwent a period of herxheimer detoxifying reactions, indicating that the “bugs” were being killed off with the high oxygen tensions of HBOT.
Some testimonial experience of such patients is listed on this page.
The simple question “Should these infections be eradicated with pharmaceuticals before HBOT treatments commence?” does not have a simple answer.
Our Centers rely heavily on Lyme-literate medical specialists (LLMD) to supervise the patient during HBOT treatments and to consider the HBOT an adjunctive medication to their good medical judgment.
Because referring physicians who send their Lyme patients to HBOT Centers prescribe appropriate dosage of 100% oxygen, all of our Centers follow their prescription carefully. Our Centers dispense HBOT at the appropriate pressures and for the length of time required to saturate the body, namely, one hour and fifteen minutes at the treatment depth.
With the time required for comfortable and safe pressurization and then return to room pressure, patients usually spend ninety minutes in the chamber at treatment pressures of at least 2.4 ATA (20 psig) to 2.7 ATA (26 psig), the pressure (dose of HBOT) dependent on the referring physician.
Most of the Lyme Disease patients treated have regained their health and eradicated Bb symptoms with 40 consecutive daily HBOT sessions of :90 minutes. In some instances, dramatically ill patients recovered in as little as 26 HBOT sessions.
How many HBOT Tx. are needed to get positive results?
Between 26 and 40 if HBOT Tx are on consecutive days. This is sometimes a controversial point amongst HBOT specialist physicians.
Our observations are as follows:
• Lyme Disease patients (aka CLD/PLS”) are all idiosyncratic (unique to each patient) and present with symptoms ranging from paraplegia to paralysis of vocal chords.
• PLS patients often are rid of B.b but still face long rehabilitation from their illness.
• Almost all PLS patients have been misdiagnosed with multiple sclerosis (MS) and Lou Gherig’s disease (ALS) because of the symptoms.
The simple answer to the question “How many HBOT sessions are needed to get positive results” cannot be defined at this time. CLD/PLS is idiosyncratic and HBOT session requirements will be influenced by multiple factors and decided upon by the supervising physician.
There is considerable discussion between registered physicians (M.D., D.O.) who claim to be “Lyme Literate Physicians” (LLP) as to HBOT Tx. pressures and whether such Tx. should be consecutive daily Tx.
For example, one published physician who claims to be a “hyperbaric specialist” recommends Tx. pressures of just under 2 ATA and five days Tx. out of each seven, with weekends off. That Center suggests that the PLS patient have forty HBOT Tx (5 /7 days) and then a break of one month and then another forty HBOT Tx (5/7 days) to obtain “complete resolution of PLS symptoms” and to “prevent the patient from becoming toxic from breathing high density oxygen.” Unfortunately, this dogmatic opinion is being accepted as “truth” by some.
We repeat the statement from the previous section:
Most of the Lyme Disease patients treated at our Centers have regained their health and eradicated Bb symptoms with 40 consecutive daily HBOT sessions of :90 minutes. In some instances, dramatically ill patients recovered in as little as 26 HBOT sessions.
If HBOT Tx. are given on consecutive days with no breaks, will the patient be endangered?
Not at all. Transient myopic changes can occur with older patients, however normal vision returns quickly.
From treating dozens of PLS patients at our affiliated centers, our observations are as follows:
• Most PLS patients treated at our Centers suffer from temporary vision changes (myopia) from the lens of the eye scavenging oxygen from the high density within the chamber. There has not been one time when eyesight did not return to normal within three weeks of cessation of HBOT Tx.
• There is ample testimony from patients that all adverse events from consecutive daily treatments (up to 40 days) reverses itself.
A “show me the science” comment on “toxicity from consecutive daily treatments” comes from Stephen Thom, MD, PhD, Professor of Emergency Medicine at the University of Pennsylvania School of Medicine:
“Aural barotrauma occurs in a small number of patients, and rare occurrences of biochemical O2 toxicity to eyes, lungs, and the central nervous system are virtually always reversible.”
Professor Thom is the lead author in “Stem cell mobilization by hyperbaric oxygen” – American Journal of Physiology-Heart and Circulation Physiology, 290:1378-1386, 2006. First published Nov 18, 2005; Research funded by the National Institute of Health.
OUR CENTERS CAREFULLY FOLLOW THE Rx OF PHYSICIANS (PACING AND Tx. PRESSURE) TO OBTAIN THE BEST OUTCOMES AT THE LOWEST COSTS (REDUCED AMOUNT OF HBOT Tx.) FOR OUR PATIENTS.
We leave the last comment on giving weekend breaks of two days to one of our specialist physicians, Doctor Brenton Wynn M.D. – Medical Director at the San Diego Center:
“When I prescribe antibiotics or other medications – some of which are highly toxic – I never tell the patient to only take them five days out of seven. In fact, I always caution and counsel the patient not to miss a dose. Likewise with HBOT, to give pause to the onslaught on the Bb spirochetes would be giving them a chance to regroup or even modify their behavior by going into their classic defense – cystic formation. HBOT should be administered according to the prescribing MD’s prescription.” Brenton Wynn, M.D.
What is the most appropriate HBOT Tx. pressure for the treatment of PLS patients?
The Fife Study advocates 2.36 – 2.8 ata.
In view of the discussion and controversy regarding higher HBOT Tx. pressures for CLD/PLS patients and the statement (made in the last question) regarding patients suffering oxygen toxicity when exposed to higher density oxygen (pressure) the following questions are appropriate:
• What is the most appropriate treatment pressure for CLD/PLS patients? and,
• Will treating CLD/ PLS patients at higher pressures cause lasting damage?
We discussed this question with members of or Scientific Advisory Board and the general consensus was as follows:
• Higher pressures cause increased free radical (Reactive Oxygen Species or “ROS”) production in the body and a toxicity.
• These ROS are swept away by the patient’s own “push-pull switches” within the body, particularly the cells producing super oxide dismutase during the twenty hour period between consecutive daily HBOT Tx.
• The patient can be further protected from ROS damage by supplemental vitamin C, Co-Q-10, and other free radical scavengers during their course of HBOT Tx.
• Chromosomal damage is reversible.
• Antibiotics (Abx.) are all toxic to both the body and the bugs they are designed to kill.
• HBOT acts synergistically with Abx. and often allow the supervising physician to reduce (titrate) the Abx. and pain killing medications given to the patient.
In summary:
It is our observation that patients do better with consecutive daily Tx at deeper pressures.
It is our belief that, to suggest to a patient that 80 HBOT Tx. spread over a 14 week period is a high resource output (time and $$) for the patient and this can be dramatically reduced with appropriate pacing, treatment depths and constant medical supervision during the treatment period.
We recommend that you review the following information on Oxygen Toxicity.
Will the so-called low pressure mild-hyperbaric (mHBOT) therapy, as administered in an inflatable bag chamber cure Lyme Disease?
Absolutely NO. Even when pressurized with 100% oxygen, the bag is useless and will not alter the progression of this disease or affect the bacteria causing it.
A number of Lyme patients had already purchased and used these inflatable devices for many months before they finally gave up and came to the HBOT Centers for treatment at the appropriate pressure of 100% oxygen.
There is much discussion on the merits of what are becoming to be called “hard chambers” and “soft chambers”. A number of medical doctors and other health practitioners such as chiropractors use the “soft” inflatable chambers and claim excellent results. However, other specialist physicians dispute the efficacy of inflatable chambers, so called “mild-hyperbarics” (mHBOT) because they do not use oxygen but merely increase room air pressure to about 3 to 4 psig over ambient. On the other hand, conventional “hard” chambers provide 100% oxygen at pressure prescribed by physicians and known to banish the many symptoms of the Bb Lyme spirochete.
Our affiliated Centers do not use nor sponsor the use of mHBOT inflatable chambers for a number of reasons. Laws of Physics do not support the claims of mHBOT advocates. Click here for more information on the laws of physics that apply to HBOT.
Also, our clinic has treated a number of patients that already undergone dozens of treatments in inflatable mHBOT chambers with no observable quantitative or qualitative positive changes in their Lyme Disease. After being treated in our conventional “hard” HBOT chambers at the correct pressures and for the appropriate treatment times, these patients showed rapid return to normal health.
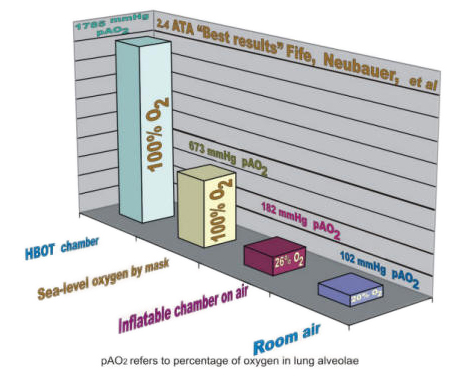
The graph clearly shows that 100% oxygen by mask at sea level delivers almost four times more oxygen to the patient than an inflatable chamber can deliver. However, to achieve the results of Fife and Neubauer in the treatment of Lyme Disease, almost three times more than 100% sea-level oxygen is required and this can only be accomplished in our conventional “hard” hyperbaric chambers.
Note: Regarding inflatable air-bag chambers: Recent media attention to the so called “mild HBOT” inflatable air-bag chambers is misleading. We believe these devices cannot be adequately pressurized and are a waste of time and money to their users. They ARE NOT Hyperbaric Oxygen Chambers. They CAN NOT provide the healing effects of hyperbaric chambers where the patient breathes 100% oxygen.
Before making a decision to use one of these devices for your treatment, check out the science and the facts … Hard vs Soft Chambers.






Patient Testimonials
These patients' battle with Lyme Disease became life-threatening. During the struggle to survive, all suffered from a diversity of misdiagnosis from specialists and suffered the consequences of following well-meaning, but incorrect, medical opinion and advice.
Ana
International cooperation was needed to assist in a life-threatening emergency. Clinicians will find the full details of recovery particularly useful.
Crystal
Crystal became ill in 1999 and did not recover fully until 2005. Her story, her "song", is both informative and encouraging for those who have almost given up hope.
Megan
'Why I travelled all the way from Florida to San Diego to get rid of Lyme Disease'